

> Abstract
Squamous cell carcinoma (SCC) of the nasal planum is a malignant neoplasm commonly seen in older cats. Long-term ultraviolet light exposure and light pigmentation or depigmentation and sparsely-haired skin are considered main risk factors for SCC. This tumour can be slowly progressive and locally invasive with a low rate of metastasis to the regional lymph nodes or lungs. Skin lesions are characterized by erythema, crusts, erosions or deep ulcers. Diagnosis is based on history and physical examination and can be confirmed by histopathological examination of the skin. Nosectomy is the recommended treatment for the invasive SCC. Prognosis is usually good to excellent with good cosmetic results in completely resected tumours.
> Epidemiology, incidence and risk factors
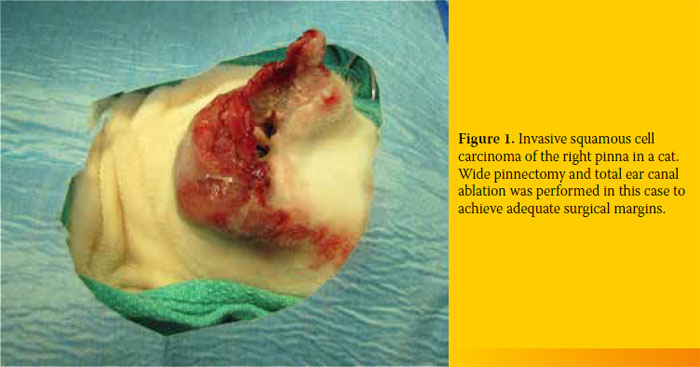
Squamous cell carcinoma of the nasal planum is a malignant tumour commonly seen in cats that derives from squamous epithelium of the skin. Pinnae, eyelids and lips are other common locations for SCC (Figure 1).1,2 White domestic short-haired cats with a median age of 12 years are affected.1 Siamese are very rarely affected, possibly due to their dark coloured skin.1,2 Overall, cats with white or lightly pigmented skin that spend most of their time outdoors exposed to ultraviolet light are predisposed to the development of SCC.1,2 Papillomavirus infection has been associated with multicentric SCC in situ but there is limited evidence that it constitutes a risk factor for the development of SCC.3,4
> Pathology and biologic behaviour of SCC
Squamous cell carcinoma is the most common tumour of the nasal planum. These tumours can be locally invasive but only rarely, in advanced or poorly differentiated states, do they metastasize to the regional lymph nodes or lungs.1,5 Three forms of SCC may be encountered depending on the time of the initial biopsy: carcinoma in situ, superficial SCC (<2 mm deep) and deeply infiltrative SCC.4,6 Carcinoma in situ or solar keratosis is a pre-malignant form of SCC composed of dysplastic cells that do not invade the basement membrane.6 More than 50% of cats with SCC of the nasal planum develop mutations of tumour suppressor gene p53 associated with ultraviolet light exposure.7 The protein (p53) that is encoded by this gene regulates the repair of the DNA damage in the cell. If DNA damage cannot be repaired, p53 will result in cell apoptosis.7
> History and clinical signs
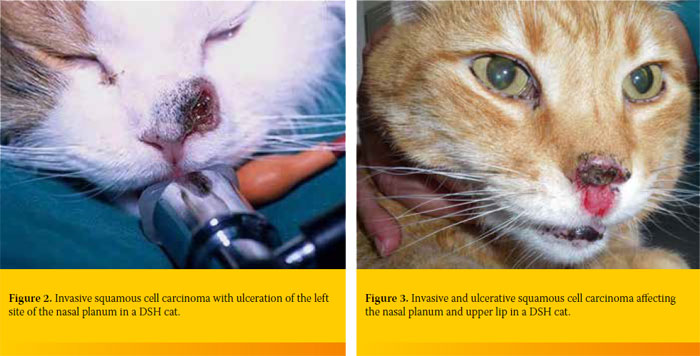
Squamous cell carcinoma is a slowly progressive disease with a median duration of clinical signs of five months ranging from weeks to years.1 In cases of SCC of the nasal planum, clinical signs progress from erythematous crusting lesions to superficial erosions and finally deeply ulcerative lesions (Figures 2, 3, 4a, 4b).1,2,4,5 As the malignant process develops, ulceration may lead to a proliferative, raised, red plaque causing nasal bleeding. Additionally, skin lesions can be accompanied by rhinitis, nasal discharge and intensive sneezing. Secondary bacterial infection is typical of deep lesions and can cause pruritus and self-traumatic lesions. Generally, regional lymph nodes are enlarged due to secondary inflammation. In cats, SCC manifests less often as a papillary to nodular mass described in dogs.2,6 In the authors’ experience, this form is rarely encountered in the nasal planum.

> Diagnosis
A tentative diagnosis of SCC is commonly made based on the history and clinical signs.4,5,8 Cytological examination can be useful but impression smears from ulcerative lesions are often non-diagnostic. An incisional deep biopsy performed under short anaesthesia may be justified for erosive or proliferative lesions to determine their invasiveness and provide a definite diagnosis.4,8
> Differential diagnosis
Squamous cell carcinoma may be differentiated from other diseases of the nasal planum including neoplasms (such as basal cell carcinoma, melanoma, fibroma, fibrosarcoma, haemangioma, haemangiosarcoma and mast cell tumour), nasal cryptococcosis, eosinophilic granuloma and early cases of pemphigus foliaceous and discoid lupus erythematosus (Figure 5).1,2,4,8 However, the appearance and distribution of accompanied skin lesions along with possible systemic clinical signs can help in differentiating the above immunemediated diseases. In all other cases, the history and other diagnostic procedures, especially skin biopsy, can confirm diagnosis.

> Clinical staging
Tumour staging should be implemented before surgical treatment. Complete staging of nasal planum tumours includes heamatological and serum biochemistry examination, cytological examination with fine needle aspiration of regional lymph nodes and thoracic radiographs. However, lymph nodes are usually involved in advanced disease, and thoracic radiographs are consistently unrewarding for the detection of metastases.1,4 World Health Organization staging of feline nasal SCC is presented in Table 1.9
| Table 1. World Health Organization staging of feline nasal squamous cell carcinoma 9 | |
|---|---|
| GRADE | DESCRIPTION |
| Tis | Carcinoma in situ (superficial ulcerative/crusting lesion not extending through the basement membrane) |
| T1a | Larger lesion <1.5 cm, exophytic |
| T1b | Larger lesion > 1.5 cm, superficial or minimally invasive |
| T2 | Ulcerative or infiltrative lesion ≥2cm |
| T3 | Larger lesion 2-5 cm or with invasion of subcutis |
| T4 | Invading muscle, bone or fascia |
> Surgical treatment
Nosectomy (nasal planum amputation or planectomy) entails a 3600 excision of the epithelium and cartilage of the nasal planum along with turbinate transection. Nosectomy is recommended as the best approach for the treatment of invasive SCC of the nasal planum.1,4,5,10 Nosectomy is a simple, quick, efficient and costeffective surgical procedure with acceptable cosmetic results.1,10 It allows surgical margin examination and achieves local tumour control with excellent long-term outcome when clean margins are obtained.1,4,5,10
 > Surgical anatomy of the nasal planum
> Surgical anatomy of the nasal planum
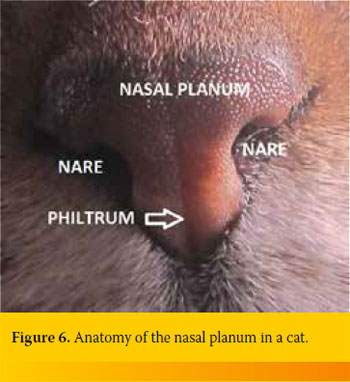
Thorough knowledge of the anatomy of the nasal planum is imperative for a successful nosectomy. The nasal planum or external nose is the pigmented, devoid of hair, flattened front portion of the nose composed of modified skin that harbours the nares or nostrils. The nares are symmetrically located in the lateral margins of the nasal planum and open into small chambers in the nasal vestibules. In the cat, the nasal planum is smaller and triangular in shape compared to the dog. The philtrum represents a median external groove that divides the upper lip and partially the nasal planum. The cartilaginous septum separates the right and left nasal vestibule and caudally this division becomes a bony septum originating from the ethmoidal crest. The paired dorsolateral nasal cartilages constitute the wings of the nostrils (Figure 6). The nasal planum is supplied by an extensive capillary network.11
> Surgical procedure
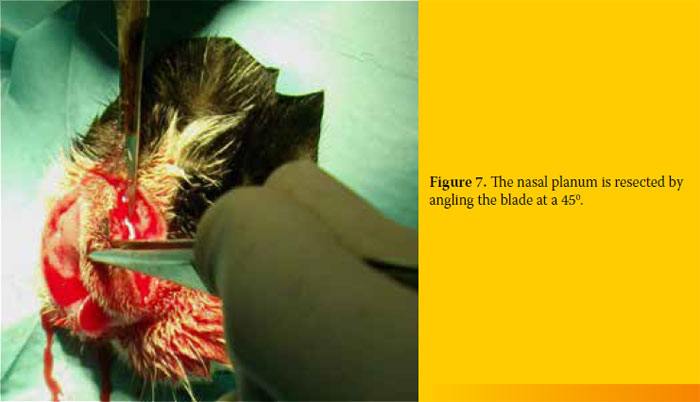
For nosectomy the cat is anaesthetized and placed in sternal recumbency with the head elevated and symmetrically positioned over a sandbag. Preoperative analgesia with infraorbital nerve blocks using bupivacaine in combination with opioids and nonsteroidal anti-inflammatory drugs and antibiotic prophylaxis is provided.5 Hair around the nasal planum and lips is clipped but the whiskers are preserved. Palpation is used to determine the tumour extension beyond the nasal planum and to estimate the proposed line of incision and lateral surgical margins which should not be less than 5 mm.5,10 The junction between the cartilage and bone represents the deep surgical margin. A full thickness skin incision is made using a No. 15 blade around the planum and the tumour. Normally a small portion of skin and buccal mucosa are preserved ventrally to the philtrum if the tumour does not extend to the lip margin. The whole nasal planum along with deeper cartilage and turbinates are resected by angling the blade at 450 (Figure 7).10 Haemorrhage is profuse but can be controlled by applying digital pressure. Following nosectomy, the skin edges retract and the conchae are visible (Figure 8). Excisional biopsy is recommended for suspicious areas of tumour infiltration. Two methods of closure are described. In the former, following nosectomy, a purse-string suture of 3-0 or 4-0 polypropylene or nylon is placed through the skin around the incision line and slightly tightened to allow second intention healing to take place for closure.10,12,13 The latter technique involves skin to nasal mucosa apposition using a few simple interrupted sutures. For this procedure, 4-0 or 5-0 polypropylene or nylon sutures are required (Figures 9, 10). This technique guarantees a more functional closure and prevents stenosis of the nasal orifice.5,12 The excised tissue is inked and submitted for histopathological examination of surgical margins and tumour assessment (Figure 11).



 > Postoperative care
> Postoperative care
Nonsteroidal anti-inflammatory drugs are prescribed for a few days and patients are discharged within 24 hours. An Elizabethan collar may be used when deemed necessary. Following surgery, a scab will form over the surgical site which will be removed under sedation or short anaesthesia at suture removal in two weeks. Complete healing of the surgical site is expected in four weeks, giving the impression of a “phantom of the opera” appearance.14 Most owners consider the cosmetic result of surgery as acceptable to good (Figures 12, 13).1
> Complications
It is advisable to offer warmed, aromatic foods and appetite stimulants, because cats are often reluctant to eat for a few days after nosectomy.12,13 Additionally, some cats may develop increased sneezing episodes or sneeze blood for several days after surgery.5,13 Occasional stricture of the nasal opening is the most serious complication encountered following nosectomy.4 Wide surgical excision of the nasal septum and various other techniques can be used for surgical reconstruction.4 Tumour recurrence is rare in completely excised tumours.1 If the surgical margins following nosectomy are incomplete, adjuvant radiotherapy can be recommended.4

> Prognosis
Cats with SCC of the nasal planum that were managed with nosectomy have good to excellent prognosis.1 Median survival time and disease-free interval for cats having nosectomy is 673 days and 594 days respectively.1 Ideally, avoidance of sunlight is advised for all patients even after surgical treatment to prevent recurrence or new lesions in other non-pigmented sites. Tattooing has not been shown to decrease the incidence of SCC.4
> Other treatment modalities
Superficial SCC of the nasal planum can also be successfully treated using curettage and diathermy, cryosurgery, photodynamic therapy or radiotherapy including brachytherapy or teletherapy. However, treatment effectiveness assessment shows that surgical margins cannot be obtained using these techniques; consequently, recurrences are commonly seen.4,12,15,16 A detailed description of the various methods is beyond the purpose of the present review.
> References
1. Lana SE, Ogilvie GK, Withrow SJ, Straw RC, Rogers KS. Feline cutaneous squamous cell carcinoma of the nasal planum and the pinnae: 61 cases. J Am Anim Hosp Assoc 1997, 33: 329-332.
2. Clifford CA. Neoplastic and non-neoplastic tumors. In:Miller and Kirk’s Small Animal Dermatology. Miller WH, Griffin CE, Campbell KL (eds). 7th edn. Elsevier: St Louis, 2013, pp. 774-843.
3. Munday JS, Witham AI. Frequent detection of papillomavirus DNA in clinically normal skin of cats infected and noninfected with feline immunodeficiency virus Vet Dermatol, 2010, 21: 307-310.
4. Withrow SJ. Cancer of the nasal planum. In: Withrow and MacEwen’s Small Animal Clinical Oncology. Withrow SJ, Vail DM
5. Thomson M. Squamous cell carcinoma of the nasal planum in cats and dogs. Clin Tech Small Anim Pract 2007, 22: 42-45.
6. Ruslander D, Kaser-Hotz B, Sardinas JC. Cutaneous squamous cell carcinoma in cats. Compend Contin Educ Pract Vet 1997, 19: 1119-1129.
7. Teifke JP, Lohr CV. Immunohistochemical detection of p53 overexpression in paraffin wax-embedded squamous cell carcinomas of cattle, horses, cats and dogs. J Comp Pathol 1996, 114: 205-210.
8. White SD. Diseases of the nasal planum. Vet Clin North Am Small Anim Pract 1994, 24: 887-895.
9. Ladlow JF. Nose. In: Feline Soft Tissue Surgery. Langley-Hobbs SJ, Demetriou JL, Ladlow JF (eds). Saunders Elsevier:Edinburg, 2014, pp. 655-669.
10. Withrow SJ, Straw BC. Resection of the nasal planum in nine cats and five dogs. J Am Anim Hosp Assoc 1990, 26: 219-222.
11. Smith BJ. Respiratory system. In; Atlas of Feline Anatomy for Veterinarians. Hudson LC, Hamilton WP (eds). 2nd edn. Teton New Media: Jackson, 2010, pp. 137-152.
12. Ayres SA, Liptak JM. Head and neck tumors. In: Veterinary Surgical Oncology.Kudnig ST, Seguin B (eds).Wiley- Blackwell: Ames, 2012, pp. 87-117.
13. Straw RC. Resection of the nasal planum. In: Current Techniques in Small Animal Surgery. Bojrab MJ (ed). 5thedn. Teton New Media: Jackson, 2014, pp. 371-375.
14. Pavletic M. Nasal reconstruction techniques. In: Atlas of Small Animal Wound Management and Reconstructive Surgery. Pavletic M (ed). 3rd edn. Wiley-Blackwell: Ames, 2010, pp. 573-601.
15. Jarrett RH, Norman EJ, Gibson IR, Jarrett P. Curretage and diathermy: a treatment for feline nasal planum actinic dysplasia and superficial squamous cell carcinoma. J Small Anim Pract 2013, 54: 92-98.
16. Murphy S. Cutaneous squamous cell carcinoma in the cat: current understanding and treatment approaches. J Feline Med Surg 2013, 15: 401- 407.
