

Nikitas Ν. Prassinos DVM, PhD, Miltiadis Τ. Dentsas DVM, Androniki Α. Krystalli DVM
Companion Animal Clinic, School of Veterinary Medicine, Aristotle University of Thessaloniki, Thessaloniki, Greece
MeSH keywords:
cat, dog, orthopaedics
Abstract
Musculoskeletal disorders in cats are less frequent compared to dogs. However, feline orthopaedics is nowadays an independent field, proving the words “cats are not small dogs”. As a matter of fact, between the two animal species there are several differences, (e.g. anatomical, functional), of which the clinician should be aware, and they should be taken into consideration in order to succeed in diagnosing and managing various orthopaedic conditions. The independent nature of the cat often leads to risky situations and for that reason most of feline orthopaedic disorders originate from trauma. The orthopaedic examination of cats is more difficult compared to dogs and for that reason diagnosing orthopaedic problems in cats can be challenging. In conclusion, there is a trend for most of feline orthopaedic problems to be managed conservatively, however treatment should be individualised for each case.
Introduction
Ness et al. (1996) have reported that in the United Kingdom, musculoskeletal disorders in cats are considerably less frequent than in dogs, except for abscesses formed by cat bites, a fact which is considered to apply in our country as well. However, the constantly increasing number of pet cats, combined with an increase in feline life expectancy and owner demand for improved veterinary care, have all contributed to feline orthopaedics becoming a separate and independent entity of companion animal orthopaedics, which is very accurately described by the phrase “cats are not small dogs” (Scott & McLaughlin 2007a). It is therefore generally acknowledged that there are key differences between the two species, which should be taken into consideration when orthopaedic problems are investigated and managed.
It is generally believed that cats are good orthopaedic patients due to their small size, their sedentary lifestyle and their ability to redistribute their body weight in order to protect the injured limb (Emery & Murakami 1967). It is a common misconception that dealing with fractures in cats is simple and that callous formation usually occurs without complications (Richardson & Thacher 1993). In fact, it has been reported in veterinary literature that in order for feline fractures to heal, it is enough to place the bone fragments in the same room (Toombs et al., 1985). However, the above has not been clinically or experimentally substantiated, and instead cats suffer the same fracture repair complications as dogs (Schrader 1994). Perhaps, in the end, the perception that feline orthopaedics is simple, stems from the fact that cats can considerably counteract functional disorders to a satisfactory extent (Scott & McLaughlin 2007a).
Τhe obvious disadvantage of the feline small size is that it is challenging for the veterinary surgeons to locate and handle the small bones and bone fragment edges (Hill 1977). The small bones of the peripheral feline limb in particular are not easily imaged with accuracy in radiographs, resulting in difficulties during the diagnostic, manipulation and surgical restoration process. Consequently, in feline orthopaedics the proper small-sized surgical equipment and orthopaedic supplies are required (Scott & McLaughlin 2007a).
Differences between cats and dogs with orthopaedic implications
Feline temperament such as independent nature and curiosity are common reasons leading to risky situations. Traffic accidents, high-rise syndrome or trauma from bite wounds are commonly encountered in a clinical setting and may cause severe and multiple injury in the musculoskeletal system and soft tissues. Therefore, most feline orthopaedic conditions are traumatic in origin and usually affect the hind limbs, including the pelvic bones and sacral body (Voss & Steffen 2009).
Cats are often admitted with a brief history of being lost for a few days and having returned with reduced mobility and/or behavioural disorders, which are not usually evaluated by the owners as indications of pain. A thorough history should aim to confirm the possibility that trauma may have occurred, to define the time lapse between trauma and admission and to locate the body systems that may had been affected (Schaer 1994).
Cats with orthopaedic conditions can easily conceal minor to moderate musculoskeletal disorders, and lameness is less frequently observed compared to dogs. In consequence, diagnosing feline orthopaedic disorders often poses a challenge, due to its particular nature (Martin 1994).
During the feline orthopaedic examination, key problems are reluctance to walk inside the examination room and the difficulties in restraining the fractious cat. As opposed to dogs, cats cannot be guided by a collar and leash in order to observe the gait and usually refuse to move freely when they are in an unfamiliar setting (Schaer 1994). In order to transcend the above difficulties, cats can be released inside the examination room and the clinician can observe through an outside window. Care, however, should be given that there are no spots the cat can use to hide or escape. Furthermore, it can be requested that the owner bring videos that have been obtained at home (Voss & Steffen 2009). In cats as well as dogs, during walking the front limbs bear more weight than the hindlimbs, however the percentage of the overall body weight shared by the hindlimbs is greater than the corresponding percentage in dogs (Conzemius et al., 2003).
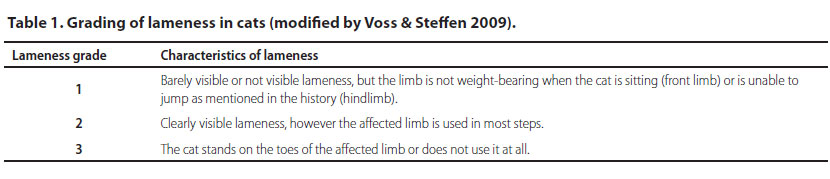
Although it is usually possible to observe a few steps of the cat, the overall evaluation of lameness can be challenging. Cats with small degrees of lameness in the front limbs can sometimes appear to walk normally, however there is no weightbearing in the affected limb when they are sitting. Cats with bilateral orthopaedic conditions may not show obvious lameness, however they are usually dull and unwilling to jump, they stand or sit with an abnormal body posture, or they walk with a flexed spine (Voss & Steffen 2009). Bilateral disorders (e.g. patellar luxation, cranial cruciate ligament rupture, hip dysplasia, hip osteoarthritis) usually affect the hindlimbs and can easily be mistaken for neurological disorders (Glass & Kent 2002). Orthopaedic disorders in more than one limbs, unstable pelvic fractures and/or vertebral fractures and subluxations should be included in the differential diagnosis, in cases when a cat cannot stand and walk after the injury (Oliver et al., 1997). In Table 1 a grading system is proposed for feline lameness (Scott & McLaughlin 2007a).
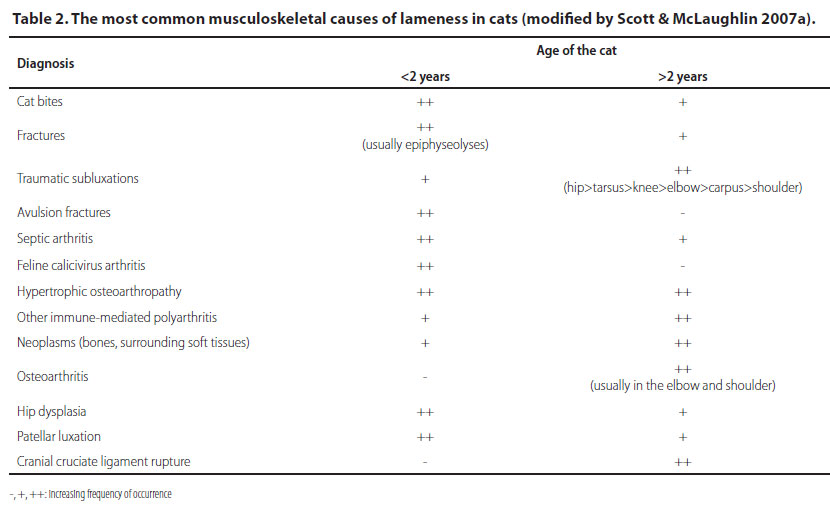
As previously mentioned, trauma is the most common cause in the differential diagnosis of feline lameness, because cats are natural explorers, but this fact should not mislead diagnosis (Glass & Kent 2002). Several conditions that lead to lameness are the same in both animal species, however their clinical significance may differ. Moreover, there are causes of lameness that are rarely or never encountered in dogs, such as alpha-mannosidosis (Hubler et al., 1997). Developmental orthopaedic disorders are much rarer in cats compared to dogs. In particular, disorders which occur more frequently in dogs, such as elbow dysplasia and avascular necrosis of the femoral head have not been reported in cats, however even the existing disorders, such as hip dysplasia and patellar luxation, may have different clinical significance (Scott & McLaughlin 2007a).
Moreover, breed predisposition is less important in cats compared to dogs, possibly because purebred cats are fewer and not so different than mixed-breed cats. Except for some congenital and inherited disorders there are very few conditions that are more commonly encountered in particular breeds, such as hip dysplasia in Maine coon cats (Scott & McLaughlin 2007b). In Table 2 the most frequent feline musculoskeletal causes of lameness are presented and summarised (Scott & McLaughlin 2007a).
Feline aggression during physical examination is usually caused by fear, the impression of being trapped and pain during manipulation of the affected sites. Fear can be reduced by ensuring a serene environment, avoiding sudden moves and using the simplest restrain techniques (Beaver 2004). Most cats can become cooperative if handled with patience and respect to their particular nature (Voss & Steffen 2009).
The evaluation of pain in cats can be challenging because the obvious signs may be very mild (Voss & Steffen 2009). Cats in pain usually are presented with reduced motor activity, sit against the far end of the carrier and avoid contact with people. They tend to resist or avoid handling and may turn aggressive (Beaver 2004). Furthermore, anorexia and weight loss may indicate pain or an inability to reach the food source, especially if it has been placed at a high spot beyond reach. Likewise, if the cat cannot reach the litter box, it may urinate or defecate in various spots in the house (Martin 1994). There is often a reluctance to move, play or jump, as well as to self-groom. More usually young cats will often move around the carrier in an aggressive manner and attack the walls and bars (Voss & Steffen 2009). In regard to diagnostic imaging, because feline bones are small and lesions are often mild, good quality radiographs are mandatory (Farrow et al., 1994). Especially for the peripheral limb, mammography film is the preferred choice (Waibl 2004).
Skeletal differences between cats and dogs
Knowledge of the anatomy and physiology of the musculoskeletal system of cats is of primary importance to the veterinary surgeon, considering that there are several smaller and certain greater differences compared to dogs (Scott & McLaughlin 2007a).
The anatomy of the feline musculoskeletal system usually reflects its size, mobility and diet (Conzemius et al., 2003). In particular, the feline musculoskeletal system is more flexible, skeletal muscles are strip-shaped and the intermediate connective tissue is looser. Cats are relatively smaller in size and have a bigger body surface to body weight ratio, resulting in a lighter skeleton. Feline long bones have a wider medullary canal and thinner cortex and the flat bones have a width of barely a few millimetres, resulting in higher risk for greenstick or complete fractures during surgical manipulations for internal or external fixation (Ness et al., 1996). Furthermore, in contrast with dogs the feline long bones are relatively straighter and tubular, and the medullary canal has the same diameter in all length, a fact which ensures the effectiveness of intramedullary fixation (Scott 2005) and placement of stainlesssteel ring fixation sutures in their metaphyses.
In contrast to dogs, skeletal differences between cat breeds are minimal, therefore it is easier to form surgical techniques, tools and surgical materials without too much variability (Scott & McLaughlin 2007a).
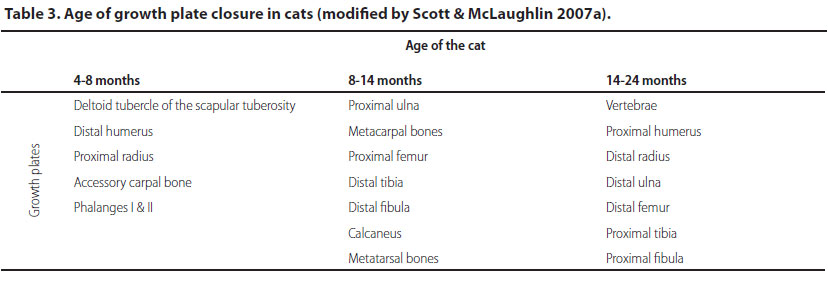
If we compare the epiphyseal growth plates between the two species, feline epiphyseal plates are plainer and more horizontal in general. As in dogs, the epiphyseal growth plate closure time is individualised and there is no particular order for growth plate fusion, however epiphyseal growth plates can be categorised in three types relative to the time of closure as it is summarised in Table 3 (Smith 1969). Epiphyseal growth plates which close late are mostly affected by delayed closure and in certain cases cartilage remnants can persist in animals older than two years. Nevertheless, in contrast to dogs, angular limb deformities are less frequent in cats, mostly due to smaller size and reduced development potential.
 .
.
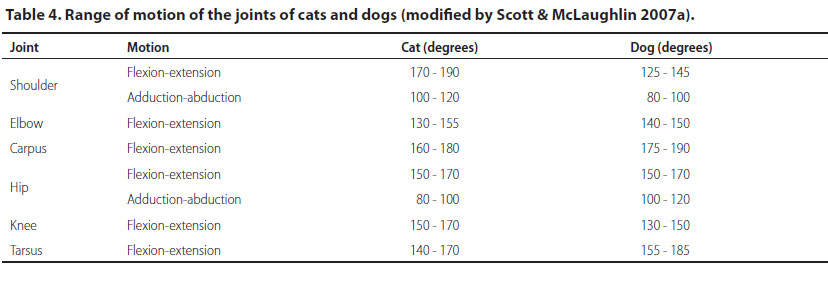
Τhe range of motion of various feline joints is different than that of dogs, and in consequence Table 4 should be consulted during the physical examination and mobility evaluation, as well as in cases of arthrodesis (Scott & McLaughlin 2007a).
i) Front limbs
The scapula of cats is broader and shorter compared to dogs (Scott & McLaughlin 2007a) and it has a tall scapular spine with two processes, the acromion and metacromion, whereas at the cranial border of the glenoid fossa there is a particularly elongated coracoid process (Figure 1). Veterinary surgeons should be aware of these processes during the surgical approach of the peripheral scapula, during retraction of the infraspinatus muscle from the scapular spine, as well as in order to avoid fractures of the coracoid process (Johnson 2014a).
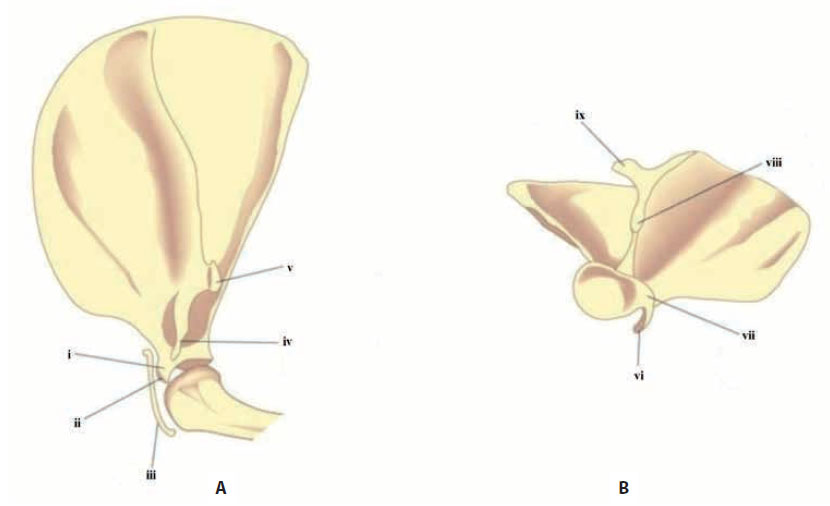
Figure 1. Lateral (Α) and ventral (Β) depiction of a feline scapula (modified from Scott & McLaughlin [2007a]). i: supraglenoid tubercle, ii: coracoid process, iii: clavicle, iv: hamate process of the acromion, v: metacromion, vi: coracoid process, vii: supraglenoid tubercle, viii: hamate process of the acromion, ix: metacromion
Cats have greater mobility in the shoulder joints compared to dogs, a fact that should not be considered abnormal during orthopaedic examination (Scott & McLaughlin 2007a).
The clavicle bone can be observed cranial to the feline shoulder joint in radiographs, which is without clinical significance, but it should not be mistaken for a scapular fracture (Figure 2). In contrast, the clavicle bone is not always observed in dogs and it is most frequently absent (Scott & McLaughlin 2007a).

Figure 2. Lateral radiograph of the shoulder joint of a cat where the clavicle can be visualised (arrow) (author’s NP patient records)
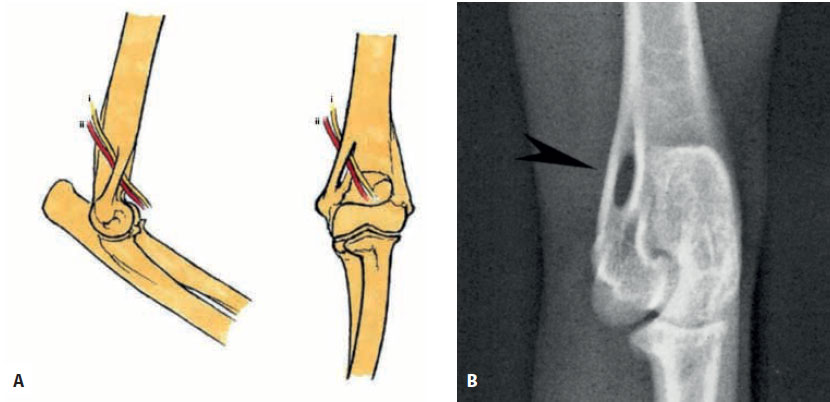
Figure 3. Α.Lateral and craniocaudal depiction of the elbow joint of a cat. Τhe median nerve and brachial artery course through the supracondylar foramen with a caudal to cranial direction (modified from Voss & Steffen [2009]). i: median nerve, ii: brachial artery. Β.Craniocaudal radiograph of the elbow joint of a cat, where the supracondylar foramen is visualised in the medial aspect of the distal humerus (arrow) (author’s NP records).
In the distal end of the feline humeral bone the supracondylar foramen can be located, in the medial aspect of the medial epicondyle, through which the median nerve and brachial artery course (Figures 3Α and 3Β). These anatomical structures are worthy of note during surgical approach and internal fixation of the distal end of the humeral bone (Johnson 2014b). Moreover, the above anatomical structures can be trapped between bone fragments in supracondylar fractures of the humeral bone, and in this case the resection of the inner wall of the foramen is required. Finally, intramedullary fixation of the humerus can be problematic due to the presence of the supracondylar foramen, due to the fact that while advancing the pin toward the distal end of the humerus, the tip can exit through the foramen and injure the median nerve and brachial artery. In order to avoid such injury, the distal end of the pin is advanced up to 7-9 mm medial to the medial epicondyle (Figure 4Α) or alternatively, if an intramedullary pin cannot stabilise the fracture due to its length, a pin of less than 1,6 mm in diameter is used, which can run through the foramen and lodge into the medial epicondyle (Schrader 1994) (Figure 4Β).

Figure 4. Α. A short, large diameter intramedullary pin is advanced up to a few millimetres medially to the supracondylar foramen in the distal diaphysis of the humerus of a cat. Β. A longer, smaller in diameter intramedullary pin is advanced up to the median epicondyle of the humerus of the cat running through the surpracondylar foramen (modified from Langley-Hobbs [2018]).
The feline ulnar nerve is located beneath the short part of the medial head of the triceps brachii muscle (Figure 5). This muscle is located caudal to the medial epicondyle of the humerus, where it inserts in the medial aspect of the olecranon. Care should be given in avoiding injury to the ulnar nerve during retraction of the muscle in order to visualise the fracture site (Johnson 2014b).
In cats, the straight shape of the distal humerus combined with the absence of a supratrochlear foramen through the olecranon fossa, results in rarer fractures in this anatomical site compared to dogs (Scott & McLaughlin 2007a).
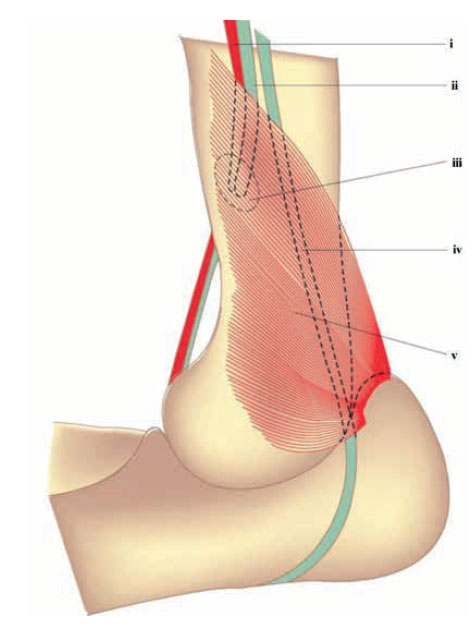
Figure 5. Depiction of the medial aspect of a feline elbow joint where the ulnar nerve course is shown (modified from Scott & McLaughlin [2007a]). i: brachial artery, ii: median nerve, iii: supracondylar foramen, iv: ulnar nerve, v: triceps brachii muscle, short segment of the medial head.
In 40% of cats there is normally a sesamoid bone in the tendon of origin of the supinator muscle. It is visible in mediolateral radiographs of the elbow joint, in the craniolateral aspect of the radial head (Figure 6) and it should not be mistaken for osteophytes or chip fractures (Wood et al., 1995).

Figure 6. Lateral radiograph of the elbow joint of a cat where the sesamoid bone in the tendon of origin of the supinator muscle of a cat can be visualised (arrow) (modified from Thrall [2016]).
Because there is greater mobility between the two antebrachium bones in comparison with dogs, fracture management by fixation of only one of them may lead to insufficient stabilisation of the other (Schrader 1994). It may be necessary to manage the fractures of both bones by surgical fixation, especially if one or both fractures are comminuted (Scott & McLaughlin 2007a). However, fixation of only one of the antebrachium bones should be avoided because the wide range of supination and pronation (45-55°), allowed by feline antebrachial anatomy, is part of the normal function of the front limb and therefore it is important to ensure the mobility between the radius and ulna, during surgical fixation of the antebrachium (Schrader 1994). From all of the above it can be derived that the ulna is more important in cats than in dogs (Scott & McLaughlin 2007a).
In cats, the distal growth plate of the ulna is horizontal (Figure 7Α), a fact that contributes to reduced frequency in post-traumatic premature growth plate closure and angular deformity of the antebrachium. In contrast, because it is “V-shaped” in dogs (Figure 7Β), the surface of ulnar cartilage is increased, resulting in increased contribution to the growth of the ulna in length, but at the same time it increases the frequency of compression injury to the stem cell layer of the ulnar cartilage (Scott & McLaughlin 2007a).
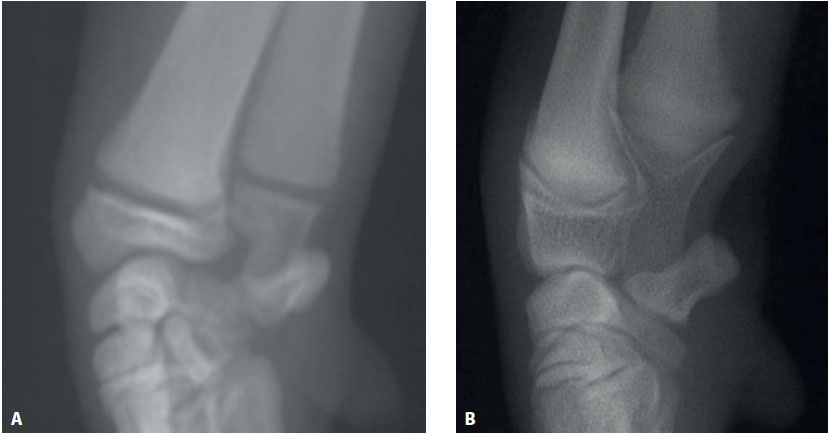
Figure 7. Craniocaudal radiograph of the distal antebrachium of a cat (Α) and a dog (Β) (author’s NP records).
ii) Hind limbs
The ligamentum teres provides a significant portion of the feline femoral head perfusion, as opposed to dogs (Culvenor et al., 1996). This might explain the fact that avascular necrosis of the femoral head has not been observed in cats. Moreover, femoral head perfusion through the ligamentum teres provides protection from possible necrosis in case of epiphysiolysis of the femoral head, resulting in good prognosis of osteosynthesis even when surgery is delayed (Scott & McLaughlin 2007a).
The muscles surrounding the hip joint present certain differences between dogs and cats, which should be taken into consideration during hip joint surgical approach. The tensor fasciae latae muscle and the vastus lateralis muscle are wider in cats. When craniolateral surgical approach of the hip is selected (Johnson 2014c), a technique most often used in cats, a wider incision is required through the tendon of origin of the deep gluteal fascia compared to dogs (Ablin & Gambardella 1991). Furthermore, in cats the gluteal muscles are larger, rendering the surgical approach of the hip joint more challenging (Johnson 2014c). Finally, the vastus lateralis muscle needs more extensive subperiosteal dissection and retraction in order to accomplish adequate exposure of the femoral neck (Ablin & Gambardella 1991). The sartorius muscle, which is encountered during lateral surgical approach of the femur (Johnson 2014c), is singular in cats, whereas in dogs it has a cranial and caudal head. Furthermore, the sacrotuberous ligament is absent in cats (Scott & McLaughlin 2007a).
The main stress points of the acetabulum in cats are the central and caudal third, in contrast to dogs where the stress points are in the cranial third. Τhis fact is of primary importance for the treatment of fractures of the acetabulum in cats, for which the notion that fractures of the caudal third of the acetabulum can be managed medically should be reconsidered (Beck at al., 2005).
In cats, there are various degrees of calcification of the sesamoid bone of the medial head of the gastrocnemius muscle and the popliteus muscles (McCarthy & Wood 1989, Arnbjerg & Heje 1993). Therefore, as long as they are non-calcified, these sesamoid bones cannot be visualised in radiographs (Scott & McLaughlin 2007a). It is worthy of note that in cats the cranial cruciate ligament is broader than the caudal, a fact that is considered to be one of the factors contributing to relatively low frequency of rupture (Scavelli 1987, Umphlet 1993).
Finally, each of the two lateral ligaments of the tibiotarsal joint is comprised by two short ligaments, meaning that there is no long segment as in dogs. This should be taken into consideration when these are replaced by artificial ligaments (Scott & McLaughlin 2007a).
iii) Spinal cord
Ιn cats, the spinal cord has greater mobility than dogs, a fact that should not be misinterpreted as abnormal during the orthopaedic examination.
Τhe nuchal ligament, which in dogs extends from the spinous process of the axis to the top of the spinous process of the first thoracic vertebrae, is absent in cats. The veterinary surgeon needs to be aware of this fact when performing a dorsal approach to the cervical spine. Furthermore, the absence of supporting ligaments is the reason why the cervical spine tends to flex in feline neuromuscular disorders.
The feline spinal cord is more flexible, and this is caused in part by the fact that intervertebral disks take up more length in cats compared to dogs (20% instead of 15-17%). Even though feline intervertebral disks present the same degeneration rate such as non-chondrodystrophic dog breeds, affected cats are usually asymptomatic (Scott & McLaughlin 2007a). The feline spinal cord terminates more caudally inside the spinal column compared to dogs, and the end of the spinal cord can vary between the vertebrae Ο7-Ι3. There is small variation between individuals and breeds, however the limit is usually Ο7 for adult cats and Ι3 for kittens (Kot et al., 1994, Dyce et al., 2002). In cats there is relatively inaccurate correspondence between neurotomes and vertebrae as opposed to dogs, therefore a localized lesion tends to affect a smaller number of neurotomes.
Finally, in cats the lumbar vertebrae are longer and narrower than in dogs (Scott & McLaughlin 2007a).
Epilogue
There is a historical tendency to use medical treatment for several feline orthopaedic disorders, whereas the same problems in dogs are managed surgically (Ness at al., 1996). Even though there are times when medical treatment can be appropriate, treatment should be individualised in each case. The aim of the feline orthopaedic surgeon should be the restoration of maximum function as soon as possible, by the simplest available means (Scott & McLaughlin 2007a).
The clinician should be aware of the above differences between dogs and cats so as to take them into consideration in order to succeed in the diagnostic approach and management of various orthopaedic disorders (Voss & Steffen 2009).
It is of key importance to realise that even though cats and dogs have several conditions in common, the two species differ greatly and cats should not be managed as small dogs, a fact which is one of the most common misconceptions in a clinical setting, not just in orthopaedics but in other disciplines as well.
Conflict of interest
The authors declare no conflicts of interest.
References
- Ablin LW, Gambardella PC (1991) Orthopaedics of the feline hip. Compend Contin Educ Pract Vet 13, 592–598.
- Arnbjerg J, Heje NI (1993) Fabellae and popliteal sesamoid bones in cats. J Small Anim Pract 34, 95–98.
- Beaver BV (2004) Fractious cats and feline aggression. J Feline Med Surg 6, 13–18.
- Beck AL, Pead MJ, Draper E (2005) Regional load bearing of the feline acetabulum. J Biomech 38, 427–432.
- Conzemius MG, Horsemen CL, Gordon W, Evans R (2003) Non-invasive, objective determination of limb function in cats using pressure platform gait analysis. Abstract Thirteenth ACVS Symposium, Washington DC. Vet Surg 32, 483–484.
- Culvenor JA, Black AP, Lorkin KF, Bradley WA (1996) Repair of femoral capital physeal injuries in cats – 14 cases. Vet Comp Orthop Traumatol 9, 182–185.
- Dyce KM, Sack WO, Wensing CJG (2002) The Neck, Back, and Vertebral Column of the Dog and Cat. In: Textbook of Veterinary Anatomy. 3rd edn. WB Saunders, Philadelphia, pp. 393–402.
- Emery MA, Murakami H (1967) The features of fracture healing in cats after immediate and delayed open reduction. J Bone Joint Surg 49B, 571–579.
- Farrow CS, Green R, Shively M (1994) Cat forelimb. In: Radiology of the cat. Mosby-Year Βook, St. Louis, pp. 123-169.
- Glass EN, Kent M (2002) The clinical examination for neuromuscular disease. Vet Clin North Am Small Anim Pract 32, 1–29.
- Hill FWG (1977) A survey of bone fractures in the cat. J Small Anim Pract 18, 457–463.
- Hubler M, Arnold S, Langley-Hobbs SJ (2009) Hereditary and congenital musculoskeletal diseases. In: P. M. Montavon, K. Voss, S. J. Langley-Hobbs. Feline Orthopedic Surgery and Musculoskeletal Disease. Saunders Elsevier, Philadelphia, pp. 21-53.
- Johnson KA (2014a) The Scapula and shoulder joint. In: Piermattei’s Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat. 5th edn. Elsevier Saunders, St. Louis, pp. 118-119.
- Johnson KA (2014b) The Forelimb. In: Piermattei’s Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat. 5th edn. Elsevier Saunders, St. Louis, pp. 198-201.
- Johnson KA (2014c) The Hindlimb. In: Piermattei’s Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat. 5th edn. Elsevier Saunders, St. Louis, pp. 328-335.
- Kot W, Partlow GD, Parent J (1994) Anatomical survey of the cat’s lumbosacral spinal cord. Progr Vet Neurol 5, 162–166.
- Langley-Hobbs SJ (2018) Fractures of the humerus. In: S. A. Johnston, K. M. Tobias. Veterinary Surgery Small Animal. 2nd edn. Elsevier Saunders, St. Louis, pp. 1980-2014.
- Martin SL (1994) The domesticated cat. In: R. Sherding. The Cat. Diseases and Clinical Management. 2nd edn. Churchill Livingstone, New York, pp. 1–6.
- McCarthy PH, Wood AK (1989) Anatomical and radiological observations of the sesamoid bone of the popliteus muscle in the adult dog and cat. Anat Histol Embryol 18, 58–65.
- Ness MG, Abercromby RH, May C, Turner BM, Carmichael S (1996) A survey of orthopaedic conditions in small animal veterinary practice in Britain. Vet Comp Orthop Traumatol 9, 43–52.
- Oliver JE, Lorenz MD, Kornegay JN (1997) Neurologic history and examination. In: Handbook of veterinary neurology. 3rd edn. WB Saunders, Philadelphia, pp. 3–46.
- Richardson ER, Thacher CW (1993) Tibial fractures in cats. Compend Contin Educ Pract Vet 15, 383–394.
- Scavelli TD, Schrader SC (1987) Nonsurgical management of rupture of the cranial cruciate ligament in 18 cats. J Am Anim Hosp Assoc 23, 337–340.
- Schaer M (1994) The medical history, physical examination, and physical restraint. In: R. G. Sherding. The Cat. Diseases and Clinical Management. 2nd edn. Churchill Livingstone, New York, pp. 7–23.
- Schrader SC (1994) Orthopedic surgery. In: R. G. Sherding. The Cat. Clinical Diseases and Clinical Management. 2nd edn. Churchill- Livingstone, New York, pp. 1649–1709.
- Scott HW (2005) Repair of long bone fractures in cats. In Pract 27, 390–397.
- Scott HW, McLaughlin R (2007a) Introduction to Feline Orthopedic Surgery. In: Feline Orthopedics. Manson Publishing, London, pp. 9-16.
- Scott HW, McLaughlin R (2007b) Fractures and Disorders of the hindlimb. In: Feline Orthopedics. Manson Publishing, London, pp. 184-191.
- Smith RN (1969) Fusion of ossification centres in the cat. J Small Anim Pract 10, 523–530.
- Thrall DE (2016) The thoracic limb. In: D. E. Thrall, I. D. Robertson. Atlas of Normal Radiographic Anatomy & Anatomic Variants in the Dog and Cat. 2nd edn. Elsevier, St. Louis, pp. 90-135.
- Toombs JP, Wallace LJ, Bjorling DE, Rowland GN (1985) Evaluation of Key’s hypothesis in the feline tibia: an experimental model for augmented bone healing studies. Am J Vet Res 46, 513–517.
- Umphlet RC (1993) Feline stifle disease. Vet Clin North Am Small Anim Pract 23, 897–913.
- Voss K, Steffen F (2009) Patient assessment. In: P. M.Montavon, K. Voss, S. J. Langley-Hobbs. Feline Orthopedic Surgery and Musculoskeletal Disease. Elsevier Saunders, Philadelphia, pp. 3-19.
- Waibl H (2004). Bones and joints. In: H. Waibl, E. Mayrhofer, U. Matis, L. Brunnberg, R. Kostlin, eds. Atlas of Radiographic Anatomy of the Cat. Parey Verlag, Stuttgart, pp. 245-290.
- Wood AK, McCarthy PH, Martin IC (1995) Anatomic and radiographic appearance of a sesamoid bone in the tendon of origin of the supinator muscle in the cat. Am J Vet Res 56, 736–738.
Corresponding author:
Miltiadis Dentsas
e-mail: This email address is being protected from spambots. You need JavaScript enabled to view it.
