

> Abstract
This study describes the application of transpelvic urethrostomy in three male, domestic, shorthair cats. Two male cats, aged one and three years old, presented with micturition disorders, due to stoma stenosis, following perineal urethrostomy, indicated to treat recurrent obstruction of the lower urinary tract. The first cat had undergone a second procedure to restore the stoma stricture. The third cat, aged three, presented with urethral obstruction attributed to lithiasis at the level of the bulbourethral glands, and was admitted with micturition inability, following a failed urinary catheterisation. Transpelvic urethrostomy was selected in all three cases, as this surgical technique allows urethrostomy to be performed approximately 1 centimetre anterior to the bulbourethral glands. Post-operatively, cat No 1 occasionally presented with urinary tract infections, treated with appropriate antimicrobial medication. Cat No 2 revealed pyuria and suppuration of the surgical wound, treated with the placement of a Foley catheter and appropriate antimicrobial medication. Cat No 3 was free of symptoms post-operatively. Stoma stenosis did not occur in any of the cases.
> Introduction
Feline idiopathic lower urinary tract disease, also referred to as feline urological syndrome or feline interstitial cystitis, resembles interstitial cystitis in humans.1 The disease is frequent in cats and may cause partial or total urethral obstruction, which is treated by catheterisation. In cases where urinary catheterisation is inapplicable, as well as in cases of recurrent urethral obstruction, unresponsive to conservative treatment, perineal urethrostomy (PU) is implemented.2-5 However, in cases of urethral obstruction, where PU cannot be applied or has failed, other urethrostomy techniques have been proposed, such as prepubic urethrostomy, subpubic urethrostomy and transpelvic urethrostomy (TPU). PU and prepubic urethrostomy have been extensively described,2-13 as opposed to subpubic urethrostomy and TPU, which are poorly cited in the relevant literature.14-16
The purpose of this study is to describe the technique, the progression, the outcome and the complications of TPU in three male cats.
> Interesting cases
Case 1
A one-year-old Domestic Shorthair (DSH) male cat was admitted due to micturition disorders. The cat lived indoors along with other cats and dogs and was fully vaccinated and dewormed. Two months prior to its admission, it had undergone PU, due to recurrent lower urinary tract obstruction. However, one month post-operatively, it exhibited stranguria and dysuria, due to stricture of the urethrostomy, and underwent a corrective PU. Clinical examination identified severe stenosis of the urethrostomy. The cat’s urethra was catheterised with a 1 mmdiameter catheter, following a small incision of the fibrotic ring formed at the site of the stoma, and a TPU was performed.
Case 2
A three- year- old DSH male cat was admitted due to micturition disorders. The cat lived indoors, as well as outdoors along with other cats, and was fully vaccinated and dewormed. Four months prior to its admission it had undergone PU, due to recurrent lower urinary tract obstruction. However, two months post-operatively it presented with gradually aggravating stranguria and dysuria. When admitted, the cat had been administered enrofloxacin (5 mg/ kg/24h, po) to treat a diagnosed lower urinary tract infection. Clinical examination revealed scarring and stenosis of the urethrostomy. There was inflammation and thickening of the skin in the area surrounding the stoma (Figure 1). The urethra was catheterised, with difficulty, using a 1mm diameter catheter, and a TPU was performed.

Case 3
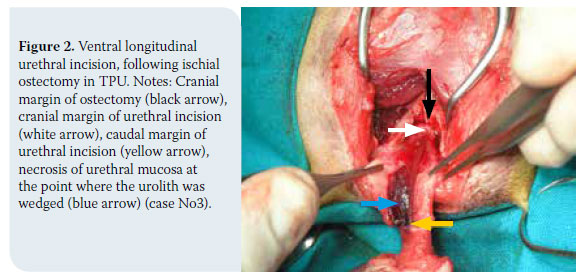
An intact DSH three-year-old cat was admitted with micturition inability, due to lower urinary tract obstruction and urolithiasis. This was the third obstruction episode in a period of two months. A few hours prior to the admission, there had been several unsuccessful attempts to catheterise the urethra. Clinical examination revealed inflammation injuries of the prepuce and penis. Subsequently, a 1mm diameter catheter was introduced into the urethra, up to the level of the bulbourethral glands, where the obstruction had been localised. The calculi were pushed back to the bladder mechanically via hydropropulsion, and the bladder was catheterised. A TPU was performed, considering the localisation of the obstruction and the expected injury of the urethra at that segment (Figure 2).
> Management
In all cases, CBC and biochemical results were within normal limits. Urinalysis revealed crystalluria, without concomitant urinary tract infection in cats No 1 and 3, and they were prophylactically administered amoxicillin-clavulanic acid (20 mg/ kg/12h, sc). Cat No 2 continued to be treated with enrofloxacin.
In all cases, medetomidine (20-40 μg/kg, im) was used for sedation, 30 minutes before anaesthesia was induced with propofol (2-4 mg/kg, iv). Following tracheal intubation, anaesthesia was maintained with isoflurane. A purse string suture was temporarily placed in the anus. The surgical procedure was performed according to Bernande and Viguier’s description (2006) in six stages.15,16
 1. Cat positioning and antisepsis
1. Cat positioning and antisepsis
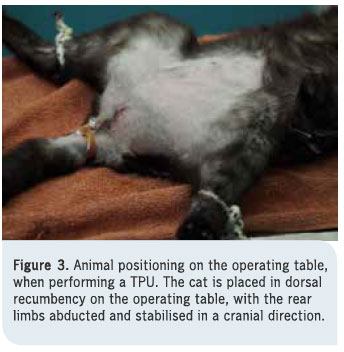
The cat is positioned in dorsal recumbency, with the rear legs secured to the surgical table in a cranial position (Figure 3). This position allows the ischiopubic symphysis to be exposed during the surgery. Subsequently, the field, which includes the base of the tail, the perineum, the posterior abdominal area, and the inner surface of the thighs, is surgically prepared (shaving, antisepsis). If a catheter has not been already introduced to the urethra, it is done at this stage.
2. Skin incision and exposure of the adductor muscles
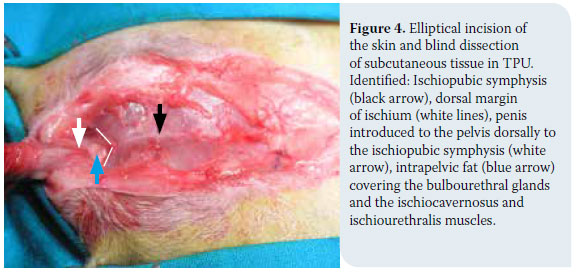
An elliptical incision is made around the scrotum and prepuce, exactly as in PU, and the incision extends cranially up to the cranial margin of the pubis. or even more anterior, in the case of an obese animal. In entire males, the testicles are then exposed and castration is performed (case No 3). Subsequently, a blind dissection of subcutaneous tissue is performed, along with the removal of a portion of subcutaneous fat in obese animals, and the ischiopubic symphysis is identified. The penis is introduced to the pelvis dorsally to the ischiopubic symphysis, which is posteriorly defined by the “V” formed by the adductor muscle fibers. The bulbourethral glands, as well as the ischiocavernosus and ischiourethralis muscles are identified and left intact (Figure 4).
3. Detachment of adductor muscles and ischial ostectomy
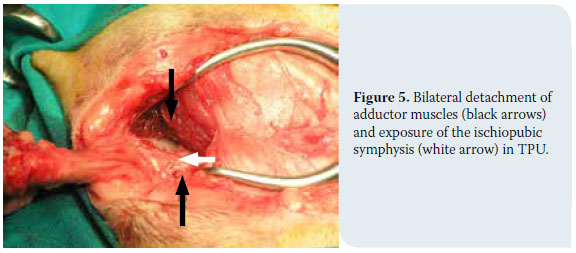
With the use of a periosteal elevator, the adductor muscles’ insertions are retracted from the ischiopubic symphysis, and its ventral part is exposed (Figure 5). Using a bone Ronguer, an approximately 12mm long and 10mm wide bilateral ischial ostectomy is performed. Attention is required so as not to include soft tissue in the excision, and so that no bone splinters remain at the edge of the osteotomy. Subsequently, the pelvic urethra is exposed and palpated, with the catheter within its canal.
4. Urethrotomy
In cases where it is impossible to catheterise the urethra pre-operatively, the urethral canal is catheterised following a partial transverse incision of the penis at the level of the bulbourethral glands. This was not necessary in any of the three cases described here, as they had been successfully catheterised pre-operatively. Subsequently, a ventral longitudinal urethral incision is made with a No 15 blade, or, preferably, with iris scissors, from the level of the bulbourethral glands, to a point 2-3 mm caudal to the cranial margin of the ostectomy. The urethrotomy should be 10-12mm long (Figure 2).
5. Urethrostomy
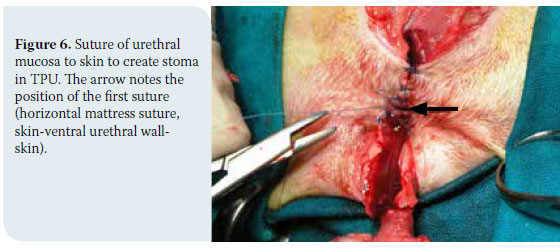
The urethral wall is manipulated with a nontraumatic DeBakey forceps. Using a nonabsorbable, monofilament, taper-point needle, 4-0 suture (e.g. Nylon, polypropylene), the urethral mucosa is sutured to the skin in a simple interrupted pattern. The suture extends from the anterior end of the stoma, with the first two sutures placed at a 45º degree angle to the mid line in a cranial direction, or with the first suture done in a horizontal mattress fashion passing twice through the ventral wall of the urethra -the latter being the suture that was applied in the three cases described here (Figure 6). The suture continues caudally on both sides of the urethra. In obese cats, it is probably required to remove fatty tissue around the stoma (case No 1), or even anteriorly (case No 3), in order to reduce suture tension. The penis distal to the bulbourethral glands is amputated, having had priorly placed a horizontal mattress suture with an absorbable, 3/0 monofilament suture at the stump of the penis for haemostasis.
6. Skin closure
The suture of the remaining incision is done in a simple interrupted pattern (Figure 7). The urinary catheter is removed and the diameter of the stoma is checked so as to ensure that a 2-2.6 mm dog catheter or a curved Mosquito haemostat (Figure 8) can be passed through it. The anal suture is removed, and, with the cat placed in a lateral position, the bladder is emptied via ventral wall pressure. Via this manipulation, in cases No 1 and 2, haemorrhagic urine was expelled, containing mucus and blood clots, and in case No 3 urine was expelled, with small, up to 3mm in diameter, calculi.


Post-operatively, in all cases an Elizabethan collar was placed to prevent self-induced injury. Enrofloxacin (5 mg/kg/24h, po) was administered for 10 days (Case No 2), and amoxicillin-clavulanic acid (20 mg/kg/12h, po) was administered for 4 days (Cases No 1 and 3). All animals were administered meloxicam (0,15 mg/kg/24h, sc) for three days. Fucidic acid ointment was applied daily on the site of the trauma, for 10 days. The sand in the litter box was replaced by newspaper, until the sutures were removed (12 days post operatively), to avoid sand covering to the urethrostomy. Chemical analysis of uroliths of Cat No 3 revealed calcium oxalate uroliths. Dietary measures were recommended for all cats, as they suffered from idiopathic lower urinary tract disease. Following suture removal, the cats were reexamined at one, three, and six months, and every time the diameter of the stoma was examined by the aforementioned methods.
> Outcome
Post-operatively, no cat presented with incontinence and all cats urinated normally within the first 24 hours. Haematuria was observed during the first three days. Cats No 1 and 3 were hospitalised for four days, and cat No 2, for ten days.
Cat No 1 has occasionally presented with haematuria and polyuria within a period of twelve years since the procedure. Each time, urine culture confirms a urinary tract infection, which is treated with the targeted antimicrobial therapy, while the psychogenic causes of cystitis recurrence are also addressed.
Cat No 2, which suffered from urinary tract infection when admitted, revealed pyuria and suppuration of the surgical wound on the third post-operative day. A Foley catheter was placed in the urethra, and replaced every 24 hours. The urine culture revealed Corynebacterium spp, which was resistant to most antimicrobial medication. Therefore, vancomycin hydrochloride (15mg/kg/8h, iv) was administered for four days, at which point the symptoms subsided and the Foley catheter was removed. Antibiotic therapy continued with the administration of linezolid (10mg/kg/8h, po) for another ten days. Two months post-operatively he presented urinary tract infection symptoms. Clinical examination did not reveal stoma stenosis. The urine culture was positive and the isolated micro-organism (Escherichia coli) was sensitive to the combination of amoxicillin and clavulanic acid, which was administered for two weeks (20 mg/kg/12h po). One week after the end of the treatment, urine culture was negative and the cat was asymptomatic for one year.
Cat No 3 was free of symptoms post-operatively.
Cats No 1, No 2, and No 3 are now aged 13, 4, and 5 respectively, and they remain asymptomatic with regard to stenosis/urethral stricture recurrence.
> Discussion
For the majority of surgeons, including ourselves, PU, as described by Wilson & Harrison (1971), is the preferred surgical technique to treat the obstructive type of feline idiopathic lower urinary tract disease.2-7 One of the most serious complications of PU is stoma stenosis, which results to similar clinical presentation as of the urethral stricture.3,17,18 It is usually suggested to perform a corrective PU to treat post-operative stenosis, yet this procedure is not always technically feasible.3,19 In this case, as well as in cases where PU is not eligible, due to a deficiency of healthy urethral tissue, prepubic urethrostomy,11 subpubic urethrostomy,14 and finally TPU15 have all been suggested.
In cases No 1 and 2, we applied TPU to restore stenosis caused by PU. Stenosis is the most serious complication of PU, and it usually occurs at the mucocutaneous margin.20 Post-operative stenosis is usually due to surgical errors, such as inadequate dissection of the urethra anterior to the bulbourethral glands, inability to mobilise the penis due to defective loosening of its junctions to the pelvis, resulting to a heightened tension upon anastomosis, urethral rupture during suturing, poor apposition of mucosa to the skin of the perineum, and post-operative rupture and/or suppuration of the surgical wound.3,17-19 In these cases, the anastomosis of the urethra to a more anterior position via TPU was preferred in lieu of performing a corrective PU, because it was impossible to identify the exact causes of the stenosis, in order to adequately treat them. Moreover, in case No 1, the cat had already undergone a corrective PU, and in case No 2, a concomitant urinary tract infection and the deteriorated state of the tissue in the area, rendered PU precarious. In case No 3, TPU was selected on grounds of insufficient healthy urethral area to perform a PU. This was due to the site and the cause of the stricture (at the level of the bulbourethral glands by a solid urolith), the visible injury of the penis, and the expected injury of the urethra at the site of the stricture, caused by the urolith and previous manipulations (Figure 6).
TPU was preferred in lieu of prepubic urethrostomy and subpubic urethrostomy in all 3 cases, as prepubic urethrostomy, which has been mostly cited in the relevant literature,11-13 is accompanied by serious, and usually irreversible complications, such as skin abrasions and necrosis, incontinence, and chronic urinary tract infections. In a study of 32 cats, which had undergone prepubic urethrostomy, one third of the cats died or were euthanised due to post-operative complications. Moreover, the owners of the cats that survived were dissatisfied, because of chronic irritant contact dermatitis at the region of the stoma.12 In a more recent study, 11 out of 16 cats who underwent prepubic urethrostomy presented with complications, and six of them were euthaniszed 1 to 23 months post-operatively.13 Subpubic urethrostomy probably presents fewer complications compared to prepubic urethrostomy, however the literature is poor.14 Additionally, it is an intensely traumatic technique, as it entails an osteotomy of the ischiopubic symphysis and a transpelvic mobilisation of the urethra.
TPU is considered a modified, less traumatic technique of subpubic urethrostomy.15 TPU has only been described in two studies by the same authors (Bernarde & Viguier 2004, 2006). In the second study, 19 cats participated, of which only 3 suffered from PU stenosis. 8 out of 19 cats presented post-operative complications. These were: rupture of surgical wound (1/19), transient incontinence (1/19), urinary tract infection (1/19), permanent or transient hair discolouration by urine (3/19), and feline idiopathic lower urinary tract disease (2/19).16
Two of our cases, for which TPU was a second or third treatment choice due to a failed PU, presented post-operative urinary tract infection, while such complication was not present in the third case, where TPU was applied as a first choice technique. Although the sample is small, this is in accord with Bernarde & Viguier study, in which, no urinary tract infection presented in any of the 16 cases where TPU was implemented as a first choice technique.16 This is possibly related to the ventral access to the urethra and the avoidance of injury of pelvic and pudendal plexus. Predisposing factors that have been identified for the presentation of urinary tract infection include the pre-operative use or overuse of catheters to establish urethral passage, idiopathic obstructive uropathy, due to feline idiopathic lower urinary tract disease, and the alterations of anatomical and functional barriers of the urethra.3,5,17,19 In one of our cases, occasional urinary tract infections were attributed to recurrent lower urinary tract disease and an ascending infection due to the loss of anatomical and functional urethral barriers. In the second case, that of the cat suffering from a urinary tract infection when operated, the suppuration of the surgical wound was attributed to the development of resistant strains. In order to prevent nosocomial infections, immediately after the infection was controlled, the catheter was removed and the cat was discharged from the clinic, continuing the appropriate antimicrobial treatment by oral administration. Despite this complication, there was no stenosis of the stoma, and this is consistent with Bernarde & Viguier’s research, according to which the rupture of the suture in one case (1/19) did not result in stenosis. In our case, two months later there was a recurrence of urinary tract infection, caused by a different microbial strain, and since then, the cat has been symptom-free. This urinary tract infection falls within the range of expected random urinary tract infections often occurring in animals that suffer from feline idiopathic urinary tract disease and that have undergone urethrostomy.6
In our cases, the skin/urethral suture was done with a synthetic (nylon), non-absorbable, 4/0 suture in an interrupted pattern. It is reported in the literature that, in PU, monofilament or multifilament absorbable sutures (polydioxanone, polyglactin 910) may also be used in simple interrupted or continuous suture patterns.21 This could be applied to TPU as well, reducing animal irritation, as well as trauma of the stoma, during suture removal.3
In case No 3, due to the severe obesity of the cat, extensive subcutaneous fat removal was required throughout the incision. While in the description of the technique16 it is generally reported that during surgical access fatty tissue is being removed from the area, limited removal of fat around the urethrostomy does not appear to adequately reduce suture tension in obese animals. In our opinion, in obese animals, the surgical incision should be longer cranially, and a sufficient amount of subcutaneous fat should be removed. This would ensure the anatomical symmetry of the area following suture of the incision, and reduce suture tension and stoma retraction. In this case, as in the other two, no stenosis of the stoma was observed, and this is in line with the literature so far. In TPU, the stoma is created approximately 15-18 mm anterior to the bulbourethral glands, where the diameter of the urethra is larger, thus contributing to prevent stenosis.
> Conclusions
TPU was performed to repair a failed PU in the case of two cats, and as a first choice surgical treatment in the case of one cat. Post-operative stenosis of the stoma did not occur in any animal, and mild, manageable complications only occurred in the two cats, which had already undergone a failed PU. In our opinion, this technique can be used in case of PU failure, as an alternative to subpubic urethrostomy and prepubic urethrostomy. Compared to PU, TPU could be the preferred technique, as, although it requires ostectomy, it allows ventral access to the urethra, reducing nerve injury in the area, which results in better functioning of the urinary system postoperatively, and in fewer complications. However, the bibliographic references that would support its suitability as an alternative to PU, to treat the obstructive form of feline idiopathic lower urinary tract disease, are still few, and its application as a first choice technique mainly concerns cases in which urethrostomy is required to be located cranially to the bulbourethral glands.
> References
Gieg JA, Chew DJ, McLoughlin MA. Παθήσεις της ουροδόχου κύ- στης. In: Saunders Εγχειρίδιο κτηνιατρικής των μικρών ζώων Birchard SJ, Sherding RG (ed) 3rd edn, Saunders: St Louis, 2006, pp. 895-914. Για την Ελληνική γλώσσα: MENDOR Editions SA 2008.
2. Smith CW Perineal urethrostomy. Vet Clin Small Anim Pract 2002, 32: 917-925.
3. Papazoglou LG, Basdani E. Perineal urethrostomy in the cat. Technique and complications. J Hellenic Vet Med Soc 2011, 62(2): 150-160.
4. Wilson GP, Harrison JW. Perineal urethrostomy in cats. J AmVet Med Assoc 1971, 159: 1789-1793.
5. Wilson GP, Kusba JK. Urethra. In: Current Techniques in Small Animal Surgery Bojrab MJ (ed) 2nd edn, Lea and Febiger, Philadelphia, 1983, pp. 325-333.
6. Flanders JA, Harvey HJ. Surgery of the urinary tract. In: The Cat Diseases and Clinical Management Sherding RG (ed) 2nd edn, Churchill Living stone, New York, 1994, pp. 1825-1845.
7. Caywood DD, Raffe MR. Perspectives on surgical management of feline urethral obstruction. Vet Clin North Am Small Anim Pract 1984, 14: 677-690.
8. Goldman AC, Beckman SL. Traumatic urethral avulsion at the preputial fornix in a cat. J Am Vet Med Assoc 1989, 194: 88-90.
9. Fox SM. Surgical repair of a traumatic perineal laceration with urethral transection: a case report. J Am Anim Hosp Assoc 1990, 26: 301-304.
10. Holt PE Non-prostatic dysuria. In: Urological Disorders in the Dog and Cat. 2nd ed, Manson Publishing, London, 2008, pp. 59-90.
11. Brandley RL. Prebubic urethrostomy. An acceptable urinary diversion technique. Prob Vet Med 1989, 1: 120-127.
12. Mendham (JH). - A description and evaluation of antepubic urethrostomy in the male cat. J Small Anim Pract 1970, 11: 709- 721.
13. Baines SJ, Rennie S, White RAS Prepubic urehrostomy: a longterm study in 16 cats. Vet Surg 2001, 30: 107-113.
14. Ellison GW, Lewis DD, Boren FC. Subpubic urethrostomy to salvage a failed perineal urethrostomy in a cat. Comp Cont Educ Pract Vet 1989, 11: 946-951.
15. Bernarde A, Viguier E. Transpelvic urethrostomy in 11 cats using an ischial oeteotomy. Vet Surg 2004, 33: 246-252.
16. Bernarde A, Viguier E. Transpelvic urethrostomy (TPU) in the cat: a new technique. Prospective survey: 19 cases. The European J Comp Anim Pract. 2006, 16: 41-49.
17. Smith CW, Schiller AG. Perineal urethrostomy in the cat: a retrospective study of complications. J Am Anim Hosp Assoc 1978, 14: 225-228.
18. Bass M, Howard J, Gerber B, Messmer M. Retrospective study of indications for and outcome of perineal urethrostomy in cats. J Small Anim Pract 2005, 46: 227-231.
19. Kusba JK, Lipowitz AJ. Repair of strictures following perineal urethrostomy in the cat. J Am Anim Hosp Assoc 1982, 18: 308- 310.
20. Phillips H, Holt DE. Surgical removal of the urethral stoma following perineal urethrostomy in 11 cats: (1998-2004). J Am Anim Hosp Assoc 2006, 42: 218-222.
21. Agrodnia MD, Hauptman JG, Stanley BJ, Walshaw R. A simple continuous pattern using absorbable suture material for perineal urethrostomy in the cat:18 cases (2000-2002). J Am Anim Hosp Assoc 2004, 40: 479-483.
