

> Abstract
A rare case of congenital esophageal diverticulum in a male, intact, 2-month-old Yorkshire terrier is described in the present report. This is a congenital malformation of the esophageal wall that occurred during fetal development, resulting in incomplete formation of the lamina muscularis and, consequently, herniation of the esophageal wall and distension of the esophageal lumen. The main causes of admission included vomiting and regurgitation. This congenital defect was diagnosed based on esophageal endoscopy findings. Treatment was conservative and included the administration of metoclopramide and dietary guidelines.
> Introduction
An esophageal diverticulum is the herniation of a segment of the oesophageal wall, forming a type of clearly circumscribed pouch that changes the normal motility of the esophageal wall.1,2,3 It can be congenital or acquired as concerns etiology, and may be located either in the middle segment of the thoracic esophagus or near the cardiac sphincter.1 This disorder results in the entrapment of food in the pouch created by the esophageal diverticulum, thereby causing regurgitation, mild esophagodynia and sec- ondary clinical signs of aspiration pneumonia. Predisposition for the disorder has been previously reported in the Cairn Terrier and Miniature poodle breeds. No predisposition has been reported so far regarding gender.4
Pathophysiology depends on the underlying cause. For instance, congenital diverticula are ascribed to congenital malformations. Specifi cally, due to the absence of segments of the lamina muscularis during fetal development, the esophageal wall dilates, fi nally resulting in herniation of the mucosa.2,3
Acquired diverticula can be classifi ed according to the pathogenesis those caused by traction of the esophageal wall and those due to increased intra-esophageal pressure (pulsion diverticula). Traction of the esophageal wall usually occurs at the beginning of the thoracic esophagus and can be caused by infl ammation and fi brosis surrounding the organ.2,3,5,6 The fi brous connective tissue formed externally can exert traction forces on the esophageal wall. When this is the case, the wall of the diverticulum comprises all the esophageal layers.5,7 Adhesions forming between the adventitia and nearby tissues deform the esophageal lumen, creating the diverticulum. A common cause of divertic- ular formation is the extra-esophageal abscess due to grass awns.2,3
Pulsion diverticula occur in relation to esophageal motility disorders, or when peristaltic motions of the organ are obstructed by an intraluminal post-traumatic stricture formed after deep post-traumatic ulceration due to an embedded foreign body (e.g. bone fragment) in the thoracic esophagus.2,3,5,6 This process requires a few days to complete. Initially the foreign body is removed and a deep post-traumatic ulceration is noted in the location where it had been embedded, the healing of which usually leads to the formation of a stricture in the esophageal lumen. Other predisposing factors include esophagitis, megaesophagus, vascular ring anomaly and hiatal hernia.2,3,7 Τhe diverticulum is formed due to herniation of the innermost mucosa and submucosa through the lamina muscularis.8 In such cases, the diverticulum is comprised of esophageal mucosa and fibrous connective tissue.7
> Case Report
A 2-month-old male intact Yorkshire terrier, weighing 0.9 kilograms, was referred to a veterinary clinic by a private practitioner; regurgitation and vomiting were the main reasons for admission. According to its history, the dog was housed indoors without other animals and was fed a commercial dry dog food. From the age of one month, episodic regurgitation began to manifest, bearing the consistency of saliva or food after meals and/or regardless of feeding times.
The primary veterinarian had taken lateral radiographs four days earlier, including both plain and barium meal studies. Based on imaging findings, the case was diagnosed as megaesophagus and medical treatment was administered (metoclopramide 0.5 mg/kg BW, every 8 or 12 hours) as well as dietary modifications (small and frequent meals of low caloric content administered by elevated feeding). The following days showed a mild improvement in the animal’s overall status. Nonetheless, the private practitioner referred the case for a second opinion, suggesting endoscopy.
According to the owner, the mood and appetite of the animal were normal and body weight was gradually increasing. Nothing abnormal was found during physical examination.
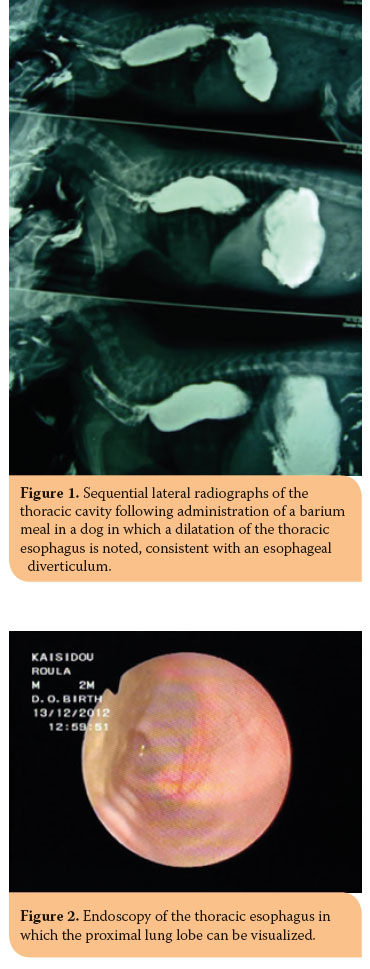 Plain lateral cervical and thoracic radiographs and barium meal studies revealed an esophageal stricture at the level of the 3rd rib anterior to the aortic arch, mild dilation of the esophageal lumen behind the stricture, and the barium meal being forwarded to the stomach (Figure 1). The above findings were consistent with an esophageal stricture, as also confirmed with fluoroscopy.
Plain lateral cervical and thoracic radiographs and barium meal studies revealed an esophageal stricture at the level of the 3rd rib anterior to the aortic arch, mild dilation of the esophageal lumen behind the stricture, and the barium meal being forwarded to the stomach (Figure 1). The above findings were consistent with an esophageal stricture, as also confirmed with fluoroscopy.
Based on the aforementioned findings, the differential diagnosis included a) congenital esophageal stricture, b) vascular ring anomaly, and c) congenital megaesophagus. In order to obtain a final diagnosis, it was decided to proceed with an esophagoscopy to which the owner gave their consent.
During esophagoscopy, (flexible OLYMPUS endoscope, vet, type XP-20) a diverticulum was revealed which occupied 2/3rds of the rostral thoracic esophagus; there were food remnants trapped in the esophageal lumen and the entire length of the lamina muscularis was undeveloped. Due to hypoplastic/ aplastic lamina muscularis, the esophageal wall was so thin and translucent that the hind left lung lobe could be clearly visualized (Figure 2). The final diagnosis was congenital diverticulum due to the hypoplastic/aplastic muscular layer of the esophageal wall.
Conservative treatment in this case included metoclopramide (at a dose of 0.4 mg/kg BW thrice daily per os 20 minutes prior to every meal) and dietary modifi cations, including the administration of low fat, liquid-type diet with the front of the dog elevated during feeding.
The owner, who was contacted by telephone six and eighteen months later, confi rmed that there were virtually no clinical signs and that physical development was normal. Recent contact with the owner revealed that regurgitation episodes were rare.
> Discussion
Congenital diverticulum is a severe and rare disorder requiring special attention as to the control and management of its negative sequelae, which mainly concern the digestive tract but also the animal’s overall status. In this particular case, the initial diagnosis was congenital megaesophagus. Referral of the case for confi rmation of the original diagnosis and management of the regurgitation episodes led to the final diagnosis of the congenital diverticulum.
Clinical signs of congenital diverticula are the typical signs of other esophageal disorders. Small diverticula are asymptomatic and usually remain undiagnosed. When the diverticulum becomes enlarged, regurgitations, esophagodynia, anorexia, fever, coughing and dyspnea develop - the latter in the case of aspiration pneumonia. Dyspnea can also be caused by pressure on the respiratory organs caused by the dilated esophageal lumen due to the amassing of food in the location of the diverticulum.1 In rare and severe cases, rupture of the diverticular wall may occur, resulting in esophageal content escaping to the mediastinum causing mediastinitis, bronchoesophageal fi stula, sepsis and systemic inflammatory response syndrome.2,3
Τhe first step in the diagnostic investigation of a case admitted due to regurgitation is radiography of the lateral cervical and thoracic areas. The latter may reveal air-filled areas or radiopaque lesions in the esophageal lumen or adjacent structures (mediastinum).2,3 In certain dog breeds, such as Shar Peis, it is possible to note small sacculations of the esophageal wall on thoracic radiographs; however, these are normal and do not usually cause clinically apparent issues.1 Any folding in the esophagus in some dogs of brachycephalic breeds should not be confused with the presence of an esophageal diverticulum. This usually occurs because in such breeds the esophagus is larger than normal, hence resembling excess tissue.2,3
Radiographs taken after the administration of a meal containing a contrast agent aim to exclude from the differential diagnosis diseases or disorders with similar radiographic appearance on plain lateral thoracic radiographs and to facilitate the diagnosis of esophageal diverticulum in particular, since they can differentiate the latter from a mass lesion located in the mediastinum or lung parenchyma which appears to be located within the esophageal lumen. Dilation of the thoracic esophagus between the heart base and the diaphragm could easily be a sign of hiatal hernia or could be an extremely rare case of gastroesophageal intussusception.2,3 In addition, a similar dilation at the level of the heart base suggests the presence of a vascular ring.1
Esophagoscopy is the gold standard in order to confi rm the diagnosis, as seen in this case. In instances where the diverticulum is not visible, it is deemed necessary to administer food and liquids to aid the diagnosis.2,3 The endoscopy excluded esophageal stenosis, which seemed to exist in the lateral thoracic radiographs after the administration of a contrast agent, and revealed a pseudostenosis due to the severe dilation of the esophagus anterior and posterior to that location. Incompatibility of endoscopic and radiographic fi ndings is attributed to the fact that radiographs are static (representing a single point in time), whereas endoscopy is a dynamic procedure and therefore more reliable in assessing the proper function of the esophageal lumen. At this point, it should be mentioned that computed tomography can possibly determine the type of an acquired diverticulum and is a less invasive procedure.7 However, in this case it was clear from the history and esophagoscopic fi ndings that the diverticulum was congenital in origin.
Metoclopramide was administered because it stimulates/modulates the motility of the gastrointestinal tract, improves esophageal contractility and increases the tone of the cardiac sphincter, thereby averting gastroesophageal refl ux. Furthermore, it has a peripheral antiemetic effect, also reducing gastroesophageal refl ux, as well as the central antiemetic action, by blocking dopaminergic receptors in the chemoreceptor trigger zone of the vomiting center which is located in the floor of the 4th ventricle.9 Consequently, metoclopramide was administered for the management of regurgitations and for its contribution to forwarding the food toward the stomach.
The other critical point of management is the addition of dietary modifi cations. More specifically, low-fat, high caloric content meals with high quality protein were recommended. It is known that fatty meals reduce esophageal contractility, whereas high protein content results in the opposite. It was recommended that meals be given twice to thrice daily so that the amount to be fed is reduced, and food should be administered by placing the animal’s food bowl on a seat or a small stairwell so that the front of the dog is higher than the back during feeding. It is suggested that the dog remain in the same position after each meal for 10-15 minutes so as to facilitate the descent of the food toward the stomach with the aid of gravity.1 Small diverticula can be managed by dietary modifi cations only, such as providing liquid or semi-liquid food, thereby reducing the possibility of it remaining in the diverticulum.3,7
At this point, it is worth mentioning the possibility of surgical management of the diverticulum. Specifi cally, in large diverticula the excess esophageal segment is removed and the esophageal wall is surgically reconstructed.1,3 In the case of a small diverticulum, surgery is mandatory only if the increase in size is due to increased endoesophageal pressure from food trapped inside the diverticulum.3 In cases where esophagitis is also present, proper medical treatment is prescribed.1 Naturally, surgical treatment is recommended in cases where there is only one esophageal diverticulum. During surgery, a lateral intercostal thoracotomy is performed at the level of the diverticulum. Defining that location is achieved by esophagography.10,11
In the present case, an esophageal diverticulum coexists with the absence of the muscle layer, which means that even with surgery the problem would persist since without the lamina muscularis, the esophagus would continue to function abnormally resulting in the formation of new diverticula as well as deterioration. Even if the segment of the esophageal wall which was defi cient regarding the muscle layer were to be removed, purely theoretically, due to its extensive length the suturing of the remaining tissue would be impractical because of excessive tension. For that reason, conservative treatment was preferred.
Absence of the muscle layer in this particular esophageal segment should be confi rmed, theoretically, not only with an endoscopy, but also with an endoscopic or full thickness surgical biopsy. The former was considered extremely dangerous because it would definitely cause rupture of the already thin wall in the area, and thoracotomy, so as to obtain a full thickness biopsy, was unattainable. Therefore, as already stated, diagnosis was based on endoscopic fi ndings (extremely thin esophageal wall, complete and clear visualization of the sinusoids of the submucosal layer and visualization of part of the left caudal lung lobe, which in the case of a normal development of the esophageal wall should not be visible, as was the case with areas before and after the esophageal diverticulum itself.
Prognosis in animals with esophageal diverticula depends on their size and etiology and consequently on management. In cases where surgical management is possible by resection of the diverticulum, prognosis is good. Prognosis is fair in cases where extensive resection is required or when a bronchoesophageal fistula is present.11 Moreover, postoperative esophageal stricture is a frequent sequela, whereas in several instances, resection of loose esopageal tissue is not feasible. In cases of traction diverticulum, prognosis depends on the cause of the extra-esophageal inflammation.2,3
Prognosis in this case was initially exceptionally poor and revaluation was programmed for a month later. Follow-up by telephone contact, at one month, six months and two years after the initial diagnosis, revealed that the dog was healthy, its appetite and growth rate were normal and regurgitation episodes were reduced and only noted when the animal consumed food not included in the veterinary recommendations.
Naturally, in the long term, prognosis remains guarded due to the diverticulum. A possible explanation for the positive outcome so far, however brief its duration may be, could be ascribed to improvement of esophageal motility as age increases. Whatever the case may be, long-term prognosis is guarded due to possible development of chronic aspiration pneumonitis.
> References
1. Ράλλης ΤΣ. Νοσήματα του οισοφάγου. Γαστρεντερολογία του σκύ- λου και της γάτας. 2η έκδ. University Studio Press: Θεσσαλονίκη, 2006, σελ. 77-105.
2. Washabau RJ, Day MJ. Esophagus. In: Canine & Feline Gastroenterology. Elsevier Saunders: Missouri, 2013, p. 595.
3. Washabau RJ. Disorders of the pharynx and oesophagus. In: Hall EJ, Simpson JW, Williams DA, editors. BSAVA Manual Canine and Feline Gastroenterology. 2nd edn. British Small Animal Association: Gloucester, 2005, pp. 143-144.
4. Nawrocki MA, Mackin AJ, McLaughlin R, Cantwell HD. Fluoroscopic and Endoscopic Localization of an esophagobronchial fi stula in a Dog. J Am Anim Hosp Assoc. 2003, 39: 257-261.
5. Hill FWG, Christie BA, Reynolds WT, Lavelle RB. An oesophageal diverticulum in a dog. Aust Vet J 1979, 55: 184-187. Συγγενής εκκολπωμάτωση οισοφάγου
6. Pearson H, Gibbs C, Kelly DF. Oesophageal diverticulum formation in the dog. J small Anim Pract 1978, 19: 341-355.
7. Glazer Α. (2014). Esophageal Diverticula in Small Animals. In: http:// www.merckmanuals.com/vet/digestive_system/diseases_of_the_ esophagus_in_small_animals/esophageal_diverticula_in_small_animals. html, (accessed 10 February 2014).
8. Park HA, Kim JW, Park HM. Characteristics of Esophageal Diverticula Using Computed Tomography and Three-Dimensional Reconstruction in a Maltese Dog. J Vet Med Sci 2012, 74: 1233-1236.
9. Ramsey I, editor-in-chief. BSAVA Manual of Small Animal Formulary. 7th edn. British Small Animal Veterinary Association: Gloucester, 2011, pp. 226-227.
10. Kyles AE. Esophagus. In: Slatter D. Textbook of Small Animal Surgery. 3rd edn. vol. I. Elsevier Health Sciences: Philadelphia, 2003, pp. 585-586.
11. Kyles AE. Esophagus. In: Tobias KM, Johnston SA, editors. Veterinary Surgery Small Animal. vol II. Elsevier Saunders: Missouri, 2012, pp. 1477- 1478.
